
She eats the same thing for lunch every day for three months, then suddenly can’t stand it. He forgets meals entirely when he’s working, then eats an entire day’s worth of food at 10pm. She’s been told she’s “picky” her whole life, but the wrong texture genuinely makes her gag.
In my experience, patterns like these often confuse the people witnessing them. They can look like stubbornness, lack of discipline, or disordered eating that should respond to the usual interventions. But for many people with ADHD, food is complicated in ways that have nothing to do with willpower. And the eating difficulties can appear long before anyone suspects ADHD might be involved.
If you’re supporting someone whose eating patterns don’t quite make sense, or if you’re trying to understand your own relationship with food, the connection between ADHD and eating is worth understanding. Many people receive eating disorder diagnoses without anyone considering that ADHD might be driving the behaviour. Others struggle for years with patterns they can’t explain, never realising that an ADHD assessment might illuminate what’s actually going on.
What Does Science Say?
The link between ADHD and eating difficulties is well documented across multiple large-scale studies.
Prevalence and Risk
A 2016 meta-analysis by Nazar and colleagues, pooling data from over 33,000 participants, found that people with ADHD are nearly four times more likely to develop an eating disorder than the general population. The risk was elevated across all types: anorexia, bulimia, and binge eating disorder.
The relationship works both ways. When researchers looked at people already diagnosed with eating disorders, they found ADHD at rates far higher than expected. For binge eating disorder specifically, the odds of having ADHD were nearly six times higher than in the general population.
| Comparison | Odds Ratio | What This Means |
| Any eating disorder in people with ADHD | 3.82x | People with ADHD are nearly 4 times more likely to develop an eating disorder |
| ADHD in people with eating disorders | 2.57x | People with eating disorders are over twice as likely to have ADHD |
| ADHD in people with binge eating disorder | 5.77x | Binge eating disorder shows the strongest link to ADHD |
Shared Neurology
Research has identified overlapping brain circuits involved in both conditions. A 2017 systematic review by Kaisari and colleagues at the University of Birmingham found consistent evidence linking ADHD symptoms to both binge-type and restrictive eating behaviours, with impulsivity emerging as a key shared mechanism. The prefrontal cortex, which governs executive function and impulse control, shows reduced activity in both ADHD and disordered eating. The reward pathways involving dopamine, particularly in the nucleus accumbens, are implicated in both the attention difficulties of ADHD and the compulsive eating patterns seen in binge eating disorder.
A 2023 longitudinal study by Martin and colleagues, also at Birmingham, found that interoceptive accuracy, the ability to perceive internal body signals like hunger and fullness, specifically mediated the relationship between ADHD symptoms and disordered eating. People with more inattentive symptoms were less able to accurately perceive their internal states, which in turn predicted both restrictive and binge-type eating patterns.
Why ADHD Affects Eating
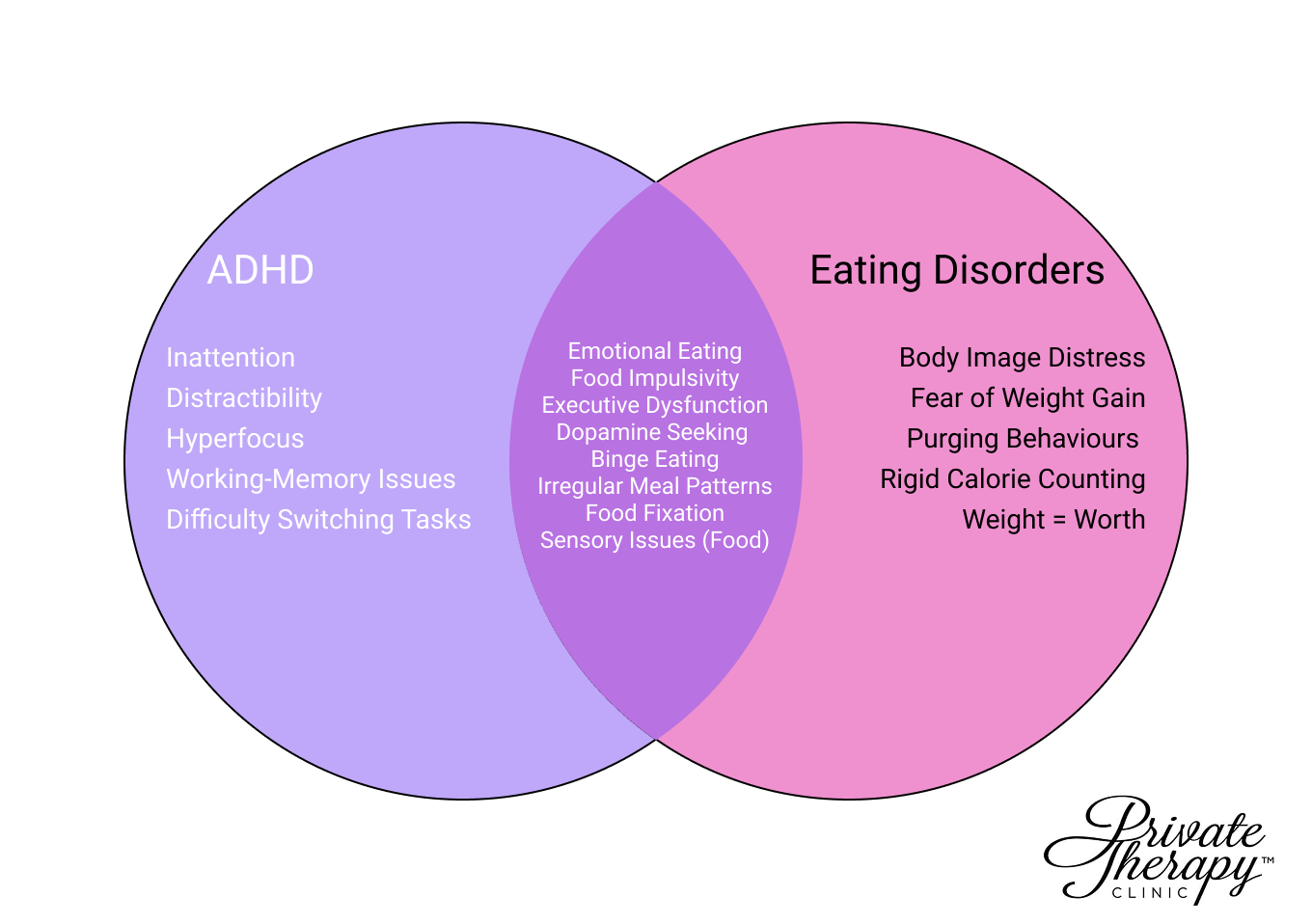 ADHD and Eating Disorder Signs VENN Diagram
ADHD and Eating Disorder Signs VENN Diagram
Several overlapping mechanisms explain why ADHD makes eating complicated. Understanding them can help make sense of patterns that might otherwise seem wilful or irrational to outside observers.
Dopamine and Reward-Seeking
The ADHD brain has lower baseline dopamine activity, particularly in the prefrontal cortex and the reward pathways that connect to it. Dopamine is the neurotransmitter that makes things feel satisfying and motivating. When it’s running low, the brain looks for ways to boost it.
Food, especially food high in sugar or fat, triggers a rapid dopamine release. This explains why many people with ADHD find themselves drawn to these foods even when they’re not hungry. It’s not about taste preference or lack of discipline. It’s the brain seeking what it needs. The problem is that this kind of eating doesn’t address the underlying dopamine deficit. It provides a brief spike, then drops off, which can drive a cycle of seeking more.
Interoception: Missing the Signals
Interoception is the brain’s ability to notice and interpret signals from inside the body. Hunger, fullness, thirst, the need to use the bathroom. For many people with ADHD, these signals don’t register clearly.
In practical terms, this means someone might not notice they’re hungry until they’re ravenous. Or they might not register fullness until they’ve eaten well past comfort. The signals are there, but the ADHD brain doesn’t always pick them up in real time. This can be particularly confusing for family members who watch someone swing between not eating at all and eating far too much in one sitting.
Executive Function and Planning
Eating regularly requires planning. Noticing hunger, deciding what to eat, obtaining the ingredients, preparing the food, and actually sitting down to eat. Each of these steps requires executive function, which is exactly what ADHD impairs.
When someone is hyperfocused on a task, the idea of breaking away to make lunch can feel genuinely impossible. Not because they don’t want to eat. Because switching tasks requires a kind of mental effort that the ADHD brain struggles to generate on demand. So they don’t eat. And by the time the hyperfocus breaks, they’re starving and reach for whatever requires the least effort.
Emotional Regulation
ADHD involves difficulty regulating emotions. Feelings hit harder and faster, and calming down takes longer. For some people, eating becomes a way to manage this. Food can soothe, distract, or provide a sensory experience that dampens emotional intensity.
This isn’t unique to ADHD. But the combination of emotional dysregulation and impulsivity means the pattern can establish itself quickly and become difficult to interrupt.
Sensory Processing
Many people with ADHD have sensory processing differences that affect eating. Certain textures feel unbearable. The wrong smell can make a food inedible. This isn’t pickiness in the way people usually mean it. It’s a genuine sensory experience that makes some foods difficult or impossible to eat.
This can lead to a limited diet, reliance on “safe foods” that always feel acceptable, and real nutritional consequences. It can also be mistaken for disordered eating when it’s actually a sensory issue that happens to involve food.
How These Patterns Present
These mechanisms don’t exist in isolation. They combine and interact, producing patterns that might look like eating disorders, subclinical difficulties, or simply a baffling relationship with food. For family members and partners, recognising these patterns can be the first step toward understanding what’s actually happening.
Binge Eating
Binge eating often emerges from the combination of dopamine-seeking, poor interoception, and impulsivity. The person doesn’t notice they’re hungry until it’s urgent, eats quickly because impulse control is harder when depleted, and the food provides a dopamine hit that’s difficult to stop chasing. From the outside, it can look like greed or lack of control. From the inside, it often feels automatic and impossible to interrupt.
Forgetting to Eat
This happens when hyperfocus overrides interoceptive signals and executive dysfunction makes meal planning feel impossible. Someone might go an entire day without eating, not because they’re restricting, but because eating simply didn’t occur to them. Partners and family members often find this bewildering, particularly when the person then eats large amounts later.
Food Fixation
Food fixation is the flip side of sensory sensitivity. When someone finds something that works, that feels right, that they can eat without friction, they want to eat it repeatedly. The same breakfast every day for months. The same dinner until suddenly, inexplicably, they can’t stand it anymore. This can look obsessive or odd, but it’s usually about reducing the cognitive and sensory load of food decisions.
The Binge-Restrict Cycle
This cycle can emerge without any intention to diet. The person forgets to eat, gets too hungry, eats rapidly past fullness, feels awful, and then finds eating the next day genuinely unappealing. It looks like restriction followed by bingeing. But it started with forgetting, not with any desire to lose weight.
ARFID
Avoidant/restrictive food intake disorder overlaps significantly with ADHD and autism. It involves eating a very limited range of foods, not because of body image concerns, but because of sensory issues, fear of negative consequences like choking, or simply a lack of interest in food. Many people with undiagnosed ADHD have been living with unrecognised ARFID for years, often dismissed as “fussy eaters” since childhood.
When It Becomes Clinical
When any of these patterns becomes severe enough to significantly impair health or daily functioning, it crosses into clinical eating disorder territory. The underlying ADHD doesn’t change the seriousness. If anything, it complicates treatment, because approaches designed for neurotypical brains don’t always work.
The Role of ADHD Medication
ADHD medication, particularly stimulants, has a complicated relationship with eating. Most stimulants suppress appetite as a side effect. This can be helpful for someone prone to impulsive eating. But it can also mean they eat even less during the day, only to experience intense hunger when the medication wears off in the evening.
This creates a specific pattern that clinicians see often: minimal eating during the day, followed by significant eating in the evening and night. It’s not about poor self-control. It’s about medication pharmacokinetics. Family members sometimes notice this pattern before the person themselves does.
Lisdexamfetamine (Elvanse) is approved for binge eating disorder as well as ADHD. A 2021 systematic review and meta-analysis by Schneider and colleagues found consistent evidence that it significantly reduces binge eating episodes, though the effect wears off as the medication leaves the system. For some people, this means binges shift to the evening rather than disappearing entirely.
Medication can be a useful tool. But it doesn’t resolve the underlying relationship between the ADHD brain and food. And for some people, particularly those who already struggle to eat enough, appetite suppression can make things worse.
Why Standard Advice Often Fails
Most advice about eating better assumes a neurotypical brain. Plan your meals. Eat mindfully. Listen to your hunger cues. Stop when you’re full.
These aren’t bad suggestions. But they require exactly the capacities that ADHD impairs:
- Planning requires executive function
- Mindful eating requires sustained attention
- Listening to hunger cues requires interoceptive accuracy
- Stopping when full requires impulse control and awareness of satiety signals
Telling someone with ADHD to “just plan their meals” is like telling someone with poor eyesight to “just see the blackboard.” The problem isn’t a lack of trying. It’s that the underlying capacity isn’t there in the same way.
This doesn’t mean nothing helps. It means the strategies need to work with the ADHD brain rather than against it. External structure rather than relying on internal cues. Environmental changes rather than willpower. Systems that reduce the number of decisions required.
For family members trying to help, this is important to understand. Frustration with “why can’t you just eat normally” tends to make things worse. The person usually can’t explain why they struggle, which adds shame to the difficulty.
When to Seek Help
Not everyone with ADHD will develop an eating disorder. Many will have a somewhat complicated relationship with food that doesn’t require clinical intervention. But certain indicators suggest it’s worth seeking professional input, whether for yourself or someone you’re concerned about.
Signs that warrant further assessment include: significant unexplained weight changes; constant preoccupation with food, either wanting it or dreading it; eating patterns that are causing physical health problems; social withdrawal related to food or eating; and the use of restriction, purging, or excessive exercise to compensate for eating.
The overlap between ADHD and eating disorders means that treatment often needs to address both. Standard eating disorder treatment that doesn’t account for ADHD may not work. And ADHD treatment that doesn’t acknowledge the eating component may leave a significant problem unaddressed.
For people who have struggled with eating patterns for years without improvement, an ADHD assessment can sometimes explain difficulties that nothing else has. Late diagnosis is common, particularly in women, and the recognition can be genuinely transformative.
A Different Understanding, Not a Life Sentence
The connection between ADHD and eating difficulties can feel like bad news at first. Another thing to manage. Another way the brain makes life harder than it needs to be.
But for many people, understanding this link is actually a relief. Years of shame about being “bad with food” start to make sense. The patterns aren’t character flaws. They’re predictable outcomes of how the ADHD brain processes hunger, reward, and planning. And once you understand the mechanism, you can work with it rather than fighting against something you were never going to win by willpower alone.
This doesn’t mean eating becomes effortless. But it does mean the right support becomes possible.
How we can Help
If you’re concerned about eating patterns in yourself or someone you care about, and you suspect ADHD might be part of the picture, we can help clarify what’s happening. Our clinicians work with adults who have both diagnosed and undiagnosed ADHD, and we offer comprehensive ADHD assessments that can illuminate whether ADHD is contributing to eating difficulties. We also work with people who have co-occurring eating disorders and ADHD. You can book a free 15-minute consultation to discuss your situation and explore what support might be appropriate.












